Exposure Assessment Tools by Routes - Dermal
Overview

An exposure route![]() exposure routeThe way a chemical pollutant enters an organism after contact, e.g., by ingestion, inhalation, or dermal absorption. is the way that a contaminant enters an individual or population after contact (IPCS, 2004). Typically, exposure occurs by one of three exposure routes-inhalation, ingestion, or dermal.
exposure routeThe way a chemical pollutant enters an organism after contact, e.g., by ingestion, inhalation, or dermal absorption. is the way that a contaminant enters an individual or population after contact (IPCS, 2004). Typically, exposure occurs by one of three exposure routes-inhalation, ingestion, or dermal.
Dermal exposure can result from skin contact with contaminated environmental media, including:
- water (e.g., during bathing, washing, swimming);
- sediment (e.g., while wading, fishing);
- outdoor soil or dust (e.g., during recreational, gardening, or construction-related activities); and
- indoor dust that has settled on carpets, floors, clothing, counter tops, or other surfaces.
Water can become contaminated via direct discharges to surface water (i.e., point sources), indirect releases, and migration to groundwater or other water sources to which people may be exposed dermally.
Soil, house dust, or other materials might become contaminated as a result of intentional application (e.g., pesticide use), deposition of particulate matter (e.g., from atmospheric pollutants), or transport from other media (e.g., water).
Human receptors could also come into contact with chemicals from consumer products directly (e.g. during use) or indirectly (e.g., chemicals that have settled on indoor or outdoor surfaces).
Estimating exposure from dermal contact requires information on:
- the concentration of the contaminant in the medium that is contacted;
- timeframe of exposure (contact frequency and duration); and
- other factors that affect dermal exposure—for example, skin surface area, dermal adherence of solids to skin, film thickness of liquids on skin, and/or residue transfer factors.
Calculations to estimate dose from dermal contact are provided in this module as are various tools available for evaluating potential exposure concentrations. Exposure scenarios, exposure factors, and guidance for assessing exposure via dermal contact are also provided.
Methods
Dermal exposure assessment is a two-step process that considers the contact between contaminant and receptor as well as absorption of the contaminant into the body through the skin. The amount of contaminant absorbed represents what is available for interaction with target tissues or organs.
The magnitude of exposure is a function of media-specific contaminant concentration, timeframe of exposure (e.g., acute, chronic), and other factors that affect dermal exposure such as skin surface area.
There are a few different ways to characterize dermal exposure and dose (U.S. EPA, 1992b):
- Potential dose is the amount of contaminant applied to skin, not all of which is actually absorbed.
- Applied dose is the amount of contaminant at the absorption barrier (e.g., skin) that can be absorbed by the body.
- Internal dose is the amount of contaminant absorbed and available for interaction with biological receptors (e.g., organs, tissues).
- Biologically effective dose is the amount of contaminant that interacts with the internal target tissue or organ.
An illustration of dermal exposure and dose is provided below.
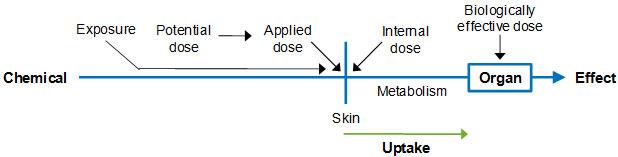 Illustration of Dermal Route: Exposure and Dose (U.S. EPA, 1992b)
Illustration of Dermal Route: Exposure and Dose (U.S. EPA, 1992b)
The potential dermal dose involves the contaminant and the matrix in which it is suspended (e.g., soil) that could come into contact with the skin. It is unlikely that all of the potential dose will come into contact with the skin. The amount of contaminant contained in a medium, such as soil, that actually comes into contact with the skin is the applied dose.
The internal dose is the amount of contaminant that gets past the exchange boundary (e.g., skin) and into the blood, or the amount of the contaminant that can interact with organs and tissues to cause biological effects (U.S. EPA, 1992b).
The internal (or absorbed) dermal dose is determined by the rate at which the contaminant is absorbed, and this will be a function of contaminant properties.
Algorithms for specific dermal pathways are provided in the Calculations tab of this module.
Calculations
Flux, or the amount of contaminant that penetrates per unit of time, has been mathematically described by Fick’s Law of Diffusion for membranes. It states that the flux of a contaminant across a homogeneous membrane is proportional to the concentration difference between the membrane outer surface and the membrane inner surface and inversely proportional to the thickness of the membrane. The key assumptions inherent in a Fick's Law based approach are:
- The skin is a homogeneous membrane.
- The flux of the contaminant across the skin is solely due to passive diffusion.
- The permeability coefficient and the flux are specific to the vehicle contacting the skin and the animal species in which they are measured.
As shown in U.S. EPA (2004), internal (absorbed) dose for inorganics in water can be calculated as follows:
DAevent = Kp x C x t
Where:
DAevent = Absorbed dose (mg/cm2-event)
Kp = Permeability coefficient (cm/hr)
C = Concentration of chemical in vehicle contacting skin (mg/cm3)
t = Time of contact (hours/event)
All parameters must be expressed in consistent units; in some cases, unit conversion factors may be necessary. This absorbed dose is generally expressed as mass of contaminant per unit surface area of skin per event (e.g., mg/cm2 event).
According to U.S. EPA (2004) the equation above may be used to estimate the absorbed dose per event (DAevent) when the inorganic contaminant contacting the skin is in the form of a liquid or aqueous mixture and the amount of contaminant on the surface is expressed as a concentration.
U.S. EPA (2004) provides alternate forms of this equation for estimating dermal exposure to organics in water. Permeability coefficients have been measured for many contaminants and can also be estimated based on correlations that use molecular weight and octanol-water partition coefficient (Kow) (U.S. EPA, 2004, 1992a).
For dermal contact with solids (e.g., soil, sediment), the concentration of contaminant contacting the skin is a function of the concentration of contaminant in the solid material (e.g., soil) and the amount of solid that adheres to the skin per unit surface area. For surface residues, the amount of chemical contacting the skin is a function of the amount of chemical on the contaminated surface and the fraction of chemical transferred to the skin.
For example, the concentration of contaminant in soil (mg/g) may be multiplied by the adherence rate (Adh) of soil to skin (g/cm2-event) to estimate the concentration of contaminant on the skin (g/cm2-event). Likewise, the concentration of contaminant on a contaminated surface (mg/cm2) may be multiplied by the transfer efficiency fraction (TF) (%/100%-event) to estimate the amount of contaminant on the surface of the skin (g/cm2-event). Absorption factors are then applied to estimate the dermally-absorbed dose per event.
Once the absorbed dose per event has been estimated, the average daily dose (ADD) can be calculated. The ADD is calculated as follows and is generally expressed as mass of contaminant per unit body weight over time (e.g., mg/kg-day).
ADDabs = DAevent x SA x EF x ED / BW x AT
Where:
ADDabs = Average daily dose (mg/kg-day)
DAevent = Absorbed dose (mg/cm2-event)
SA = Skin surface area available for contact (cm2)
EF = Exposure frequency (events/year)
ED = Exposure duration (years)
BW = Body weight (kg)
AT = Averaging time (days)
- Surface area (SA) represents the surface of the skin that is exposed
- Body weight (BW) of an individual, typically expressed in kilograms (kg), is included so that the dose is normalized to that value.
- Temporal parameters in the dose equation include:
- Exposure frequency (EF) refers to the frequency with which the exposure occurs and might be provided in events per year or events per day.
- Exposure duration (ED) is the amount of time that an individual or population is exposed to the contaminant being evaluated and is typically provided in years.
- Averaging time (AT) is the amount of time over which exposure is averaged and is equal to ED for assessing non-cancer risks. For chronic assessments (e.g., cancer), potential lifetime average daily dose (LADD) is calculated in which lifetime (LT, in days) is substituted for AT.
- Exposure parameter inputs (e.g., dermal contact factors, body weights, and relevant patterns of behavior such as timeframe of exposure) can be obtained from the Handbook.
Additional information on exposure scenarios involving the dermal route can be found in the Indirect Estimation Module of the Approaches Tool Set.
Concentrations
Sources of contamination to soil, dust, water, and sediment are discussed in the Media Tool Set. Media-specific concentrations are needed for estimating exposure via the dermal route. Data and tools that can be used to estimate concentrations are also discussed in the Media Tool Set.
Measuring Concentrations
Information on sampling techniques and analytical methods is available to support the measurement of contaminants in environmental media to which people may be exposed via dermal contact.
Modeling Concentrations
In the absence of measurement data, a variety of models can be used to estimate contaminant concentrations in soil, dust, water, sediment, or other materials to which human receptors may be exposed via dermal contact. A number of resources are available to assist in these modeling efforts.
Available Data
There are a number of information sources that provide monitoring data on contaminant concentrations in environmental media to which individuals might be exposed via dermal contact.
Scenarios
Dermal exposure can be estimated by first defining the exposure scenario![]() exposure scenarioA set of facts, assumptions, and inferences about how exposure takes place that aids the exposure assessor in evaluating or quantifying exposure. of interest. Exposure scenarios typically include information on the sources and pathways of exposure, contaminants of concern, and receptor populations. They might also describe a receptor population’s activities that may affect exposure and the timeframe over which exposure occurs.
exposure scenarioA set of facts, assumptions, and inferences about how exposure takes place that aids the exposure assessor in evaluating or quantifying exposure. of interest. Exposure scenarios typically include information on the sources and pathways of exposure, contaminants of concern, and receptor populations. They might also describe a receptor population’s activities that may affect exposure and the timeframe over which exposure occurs.
Dermal exposure could occur from contact with contaminated environmental media-soil, dust, water, sediment-or contaminants from consumer products. Dermal contact with soil could occur during outdoor recreational, gardening, or construction-related activities.
Receptors could come into contact with contaminants in soil and dust that have settled on carpets, floors, clothing, counter tops, or other surfaces. Children are particularly susceptible via this indirect pathway because certain activities (e.g., crawling or playing on the floor indoors) may increase their contact with contaminant-laden dust.
Dermal absorption of water contaminants could occur during activities such as hand washing, bathing, and swimming in a pool or surface water body. Receptors could contact contaminants in sediment while fishing, clamming, wading, or swimming in a lake, river, or other water body.
Exposure to contaminants in consumer products can occur from direct or indirect contact. For example, intentional direct contact could occur from applying cosmetics or other personal care products to the skin, or unintentional direct contact could occur from contact with laundry detergent or surface cleaner while in use. An example of indirect contact is contact with cleaning product or pesticide residues on surfaces).
The table below provides some examples of dermal exposure scenarios. The list of examples is not meant to be exhaustive. There are numerous other dermal exposure scenarios that may be constructed based on the specific needs of the assessment. There are also numerous variations of the examples provided in the table.
Additional information on exposure scenarios involving dermal exposure may be found in the Indirect Estimation Module of the Approaches Tool Set.
| Medium | Receptor Population | Activity/Timeframe | Contact Rate | Exposure Period |
|---|---|---|---|---|
| Tap water | General population; adults | Showering; lifetime | Total surface area [Table 7-1] |
Chronic |
| Surface water; localized | Children | Wading | Surface area of legs and feet [Table 7-2] |
Sub-chronic |
| Swimming pool water | Recreating adults and children | Swimming over the short-term [Table 16-1] |
Total skin surface area [Table 7-1] |
Acute |
| Soil from contaminated site | Occupational; adults | Site-specific construction occupational tenure [Table 16-8] |
Surface area of selected body parts [Table 7-2] Adherence rates [Table 7-4] |
Chronic |
| House dust | Young children | Contact during time spent indoors; less than lifetime [Table 16-1] |
Surface area of selected body parts [Table 7-2] Adherence rates [Table 7-4] |
Sub-chronic |
| Residues on indoor surfaces | Residential children | Contact during time spent indoors; less than lifetime [Table 16-1] |
Surface area of selected body parts [Table 7-2] Contact rates [Table 7-7] |
Sub-chronic |
| a Information on dermal absorption may be found in U.S. EPA’s Risk assessment guidance for Superfund: Volume I: Human Health Evaluation Manual (Part E, supplemental guidance for dermal risk assessment) (U.S. EPA, 2004). | ||||
Several resources are available that illustrate dermal exposure scenarios.
Factors
Chapter 7 of EPA’s Exposure Factors Handbook: 2011 Edition (U.S. EPA, 2011) provides information on factors that affect dermal exposure, including skin surface area, dermal adherence of solids to the skin, film thickness of liquids on the skin, transfer of contaminant residues from surfaces to the skin, and other factors. Contaminant-specific factors related to dermal absorption and internal dose, however, are not provided in Chapter 7.
Skin surface area (SA) is an estimate of the amount of skin (cm2 or m2) that can be exposed to contaminants. The more skin exposed the greater potential for dermal absorption. Depending on the scenario, total body surface area or surface areas of specific body parts may be appropriate.
Another dermal factor is the adherence factor (AF; mg/cm2), which represents the quantity of soil or solids that may adhere to the skin surface after contact. This varies with activity. Recommended values for SA and AF are provided in the Handbook.
The film thickness of liquids on skin (cm) is a measure of the amount of material that remains on the skin after contact with a liquid (e.g., consumer product such as cleaning solution or soap). Residue transfer coefficients (cm2/hour) of contaminants to human skin will vary based on exposure conditions such as activity, contact surface, and age. Recommended values for these dermal factors are not provided in the Handbook because data are limited; however, data from relevant studies are described.
The Exposure Factors Tab of the Indirect Estimation Module provides links to data on dermal contact rates.
Other activity-specific factors that might be relevant for assessing exposures with contaminants via dermal contact are available in Chapter 16 of the Handbook. These might include time spent indoors, time spent outdoors, event frequency (showers per week, swimming events per month), or time spent doing the specific activities (e.g., playing on dirt or grass, gardening, participating in outdoor recreation).
- Body weight (Chapter 8)
- Consumer product use information (Chapter 17)
- Life expectancy values, specifically when evaluating cancer risk (Chapter 18)
The Exposure Factors Tab of the Indirect Estimation Module provides links to data on other factors.
Dermal exposure factors should be selected to represent the age, gender (if appropriate), timeframe/activity level, and population group (e.g., resident, occupational worker) for the exposure scenario of interest.
EPA’s Risk Assessment Guidance for Superfund (Part E, Supplemental Guidance for Dermal Risk Assessment) (U.S. EPA, 2004) and Dermal Exposure Assessment: Principles and Applications (U.S. EPA, 1992a) provide additional guidance on the use of dermal contact parameters. Exposure factors related to dermal exposures are also described in the Soil and Dust, Water and Sediment, and Consumer Products Modules of the Media Tool Set.
Guidance
The following sources provide helpful information for conducting exposure assessments involving the dermal route of exposure.
References
- IPCS (International Programme on Chemical Safety). (2004). IPCS Risk Assessment Terminology: Part 2: IPCS Glossary of Key Exposure Assessment Terminology (122 pp, 951 K, About PDF) Exit. Geneva, Switzerland: World Health Organization.
- U.S. EPA. (1992a). Dermal Exposure Assessment: Principles and Applications (Interim Report). (EPA/600/8-91/011B). Washington, DC.
- U.S. EPA. (1992b). Guidelines for Exposure Assessment. (EPA/600/Z-92/001). Washington, DC.
- U.S. EPA. (2004). Risk Assessment Guidance for Superfund (RAGS), Volume I: Human Health Evaluation Manual, (Part E, Supplemental Guidance for Dermal Risk Assessment) Interim. (EPA/540/R/99/005). Washington, DC.
- U.S. EPA. (2011). Exposure Factors Handbook 2011 Edition. (EPA/600/R-09/052F). Washington, DC.